Preliminary data from the MILES trial, presented at AUA 2026, show that minimally invasive laser enucleation of the prostate (MiLEP) using a 22 Ch resectoscope produces significantly less early stress urinary incontinence than standard endoscopic enucleation (EEP) with a 26 Ch scope - while delivering essentially the same functional results.
The continence difference is hard to ignore: 6.5% versus 29.5% requiring at least one pad per day after catheter removal.
What the MILES Trial Did
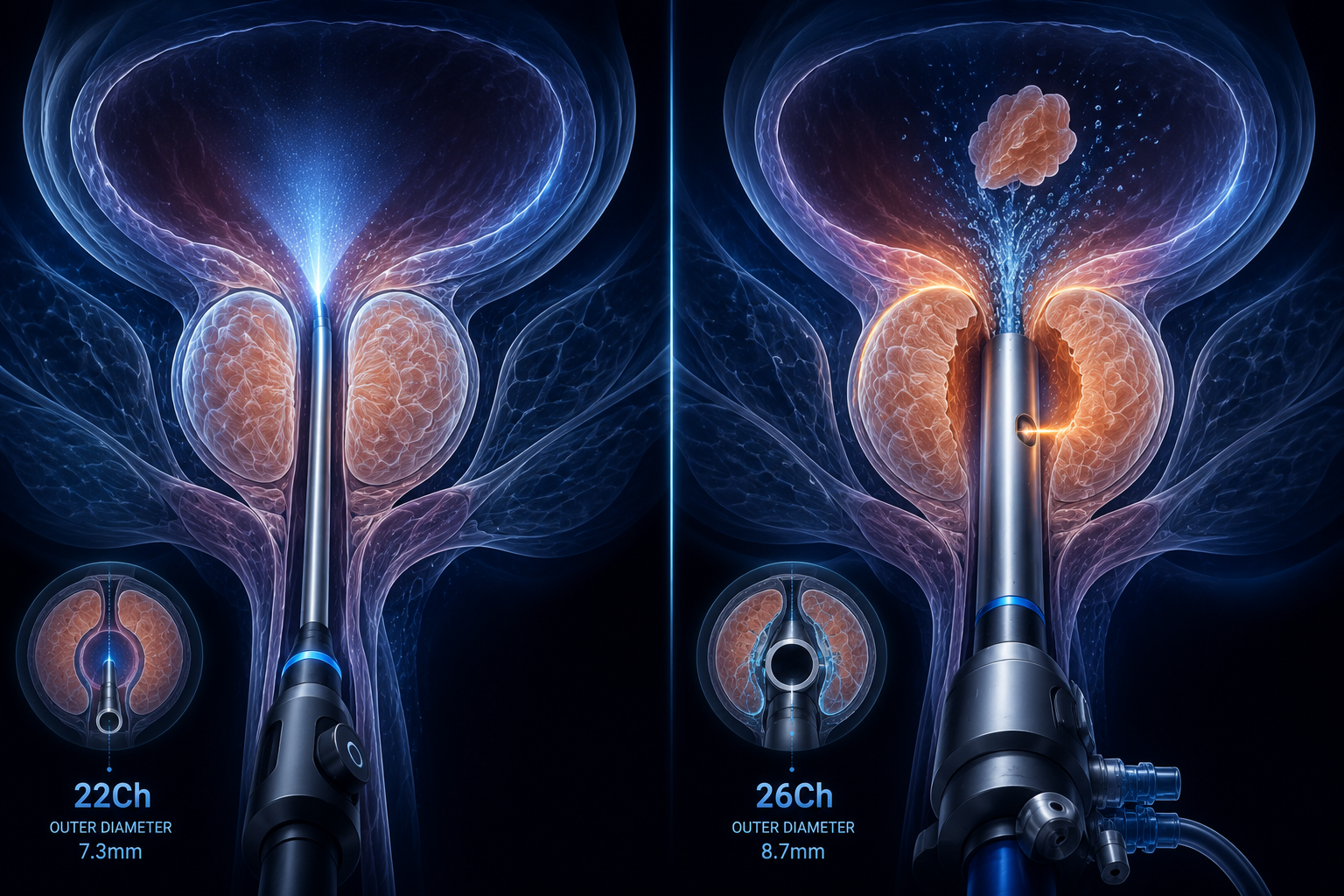
The MILES trial (NCT06839768) is a prospective randomised controlled trial comparing MiLEP (22 Ch) against standard EEP (26 Ch) in men with BPH. Both arms used the same thulium fibre laser (FiberLase U-MAX, 2J at 40 Hz) with the en bloc enucleation technique - the only variable was scope size.
Eligibility was men with prostate volumes of 30 to 150 cc, IPSS 20 or above, and Qmax 15 mL/s or below. 155 patients were included in this analysis: 77 MiLEP, 78 standard EEP. Baseline characteristics were well matched.
The primary endpoint was stress urinary incontinence after catheter removal, defined as needing at least one pad per day.
The Numbers That Matter
Everything that might make you think the smaller scope is cutting corners is equivalent between groups.
Operative time, enucleation duration, morcellation time, median tissue weight removed (34g vs 35g), catheterisation duration (1 day in both), and hospital stay (3 days in both) - all the same. At 3 months, median IPSS was 2 vs 5 (P=.27) and Qmax was 21.5 vs 23.8 mL/s (P=.99).
The difference is early SUI: 6.5% with MiLEP versus 29.5% with standard EEP (P=.04).
By 3 months, that gap has largely closed - continence rates were 100% versus 87.2%, which didn’t reach significance (P=.23). There’s also a trend in urethral strictures that hasn’t reached significance yet: 1.3% with MiLEP versus 6.4% with standard EEP (P=.06).
Why Scope Size Might Matter
The external urethral sphincter sits immediately below the prostate apex. A larger sheath passing through the external sphincter for the duration of an enucleation procedure means more mechanical stretch - and the sphincter doesn’t always recover immediately. That early SUI rate with standard EEP probably reflects transient sphincter dysfunction from instrument trauma, not from the enucleation technique itself.
The fact that both groups equalise at 3 months supports this. It’s not a permanent injury in most cases - it’s early stretch and recovery. But “you’ll be wet for a few weeks after catheter removal” is a very different consent conversation from “you’ll probably be dry.”
What We Don’t Know Yet
This is preliminary data from an ongoing trial. The primary endpoint has reached significance, but some of the secondary trends - urethral strictures especially - haven’t. Longer follow-up will matter for stricture rates, since those can present months after surgery.
We also don’t have data on whether a 22 Ch scope performs differently on larger prostates. The trial goes up to 150 cc, but the paper doesn’t break down outcomes by prostate volume. A smaller instrument working on a 140 cc gland may behave differently to the same instrument on a 40 cc gland.
And this is one trial, one centre presumably, one thulium laser platform. Reproducibility across different systems and surgeons is the next question.
Why It’s Worth Knowing About
MiLEP isn’t yet in mainstream practice - this trial is part of establishing whether it should be. But the concept matters: if you can achieve equivalent deobstruction with a smaller instrument and the patient is drier in the first weeks after catheter removal, that’s a meaningful quality of life gain.
The 3-month equalisation is reassuring from a consent perspective, but early SUI still matters. Men who go back to work, travel, or live alone don’t want to manage pads for six weeks post-surgery if they don’t have to.
Dembeck L. Minimally-Invasive Laser Enucleation for BPH Reduces Stress Urinary Incontinence. Renal and Urology News, June 2026. Data from the MILES trial (NCT06839768), presented at AUA 2026 Annual Meeting.